What Healthcare Can Learn from a Restaurant About Shift Coverage (Yes, Really.)

I used to work for Hillstone Restaurant Group.
Before you click away, stay with me. Because that experience taught me more about schedule accountability, coverage discipline, and workforce flexibility than most healthcare staffing models I’ve seen in twenty years.
Here’s how it worked:
We had fixed schedules (same shifts every week) with a minimum of three shifts per week. If we needed a day off, it was on us to find coverage, and only then would a manager approve the request.
The expectations were firm. If you called out without finding coverage, you were let go. Called out sick without documentation? Management noticed, especially when it happened on a weekend. A pattern of unverified absences carried consequences.
Harsh? Sure. But here’s the thing nobody in healthcare wants to admit:
The shifts got covered.
Not because management cracked down. Because the system had structure. And structure creates accountability.
So the important question is:
What parts of this system could work in healthcare if we adapted them correctly?
Healthcare Is Different – But Not in the Way You Think
Healthcare is licensed, regulated, high-acuity, and emotionally demanding. Patient safety is non-negotiable. You can’t just “close a section” when you’re short-staffed on a med-surg unit at 3 a.m.
But here’s the uncomfortable truth:
Many staffing problems in healthcare aren’t caused by a lack of people – they’re caused by a lack of structure.
In healthcare, where a single unfilled nursing shift can trigger overtime cascading across an entire unit, the cost per vacancy runs between $40,000 and $64,000 before you even factor in agency premiums.³
Hillstone solves coverage problems with structure. Healthcare too often relies on heroics, guilt, and last-minute scrambling.
That gap isn’t about staffing levels. It’s about systems.
What Translates to Healthcare Shift Coverage (With Guardrails)
Self-Managed Shift Coverage
In restaurants, finding your own replacement wasn’t optional, it was part of the job. You didn’t call your manager at 4 a.m. and say “I can’t come in, good luck.” You worked the phone until someone said yes.
At Hillstone, I remember spending my time during closing duties going down the contact list, calling co-workers one by one. Was it annoying? Absolutely. But it worked and it taught me that my shift was my responsibility, not just management’s problem to solve.
And here’s something healthcare leaders don’t expect from a restaurant comparison: Hillstone had its own version of acuity-based coverage.
If you worked the grill, you could only get someone else who had been trained on the grill to cover your shift. If you were one of the waitstaff who handled the financials at the end of the night, collecting reports and cash from servers and closing out registers, same rule. Only someone trained on that responsibility could take your place.
Those roles came with perks: better pay, seniority, preferred scheduling. But the tradeoff was a smaller coverage pool. Sound familiar? It should because that’s exactly how acuity works in a hospital. A med-surg nurse can’t cover a CVICU shift. A floor nurse can’t swap into a charge role without the competency. The principle is identical: specialized roles require specialized coverage.
In healthcare, this model works – if you add clinical guardrails:
- Coverage must meet licensure, unit competency, and patient acuity requirements
- Swaps require advance approval through a scheduling platform
- A digital shift-swap board or mobile app is essential (not a group text thread)
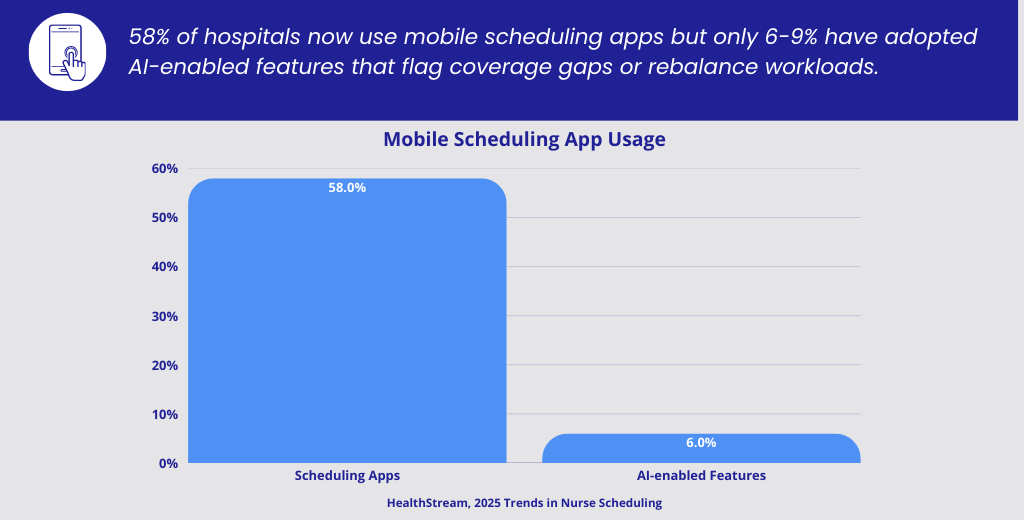
The tools exist. The adoption is lagging.
Every shift that goes unfilled because a nurse couldn’t easily post a swap costs the facility overtime, which accounts for 47% of all overtime hours worked across industries.²
The bottom line: Every time a manager is solely responsible for filling every gap, you train your staff to disengage from the schedule. Shared responsibility builds accountability and reduces burnout at the leadership level, not just the bedside.
Minimum Shift Commitments for PRN Staff
Restaurants didn’t keep people on the roster “just in case.” If you weren’t working your minimum three shifts, you weren’t on the schedule anymore.
Healthcare claims to have PRN minimums — but enforcement is often inconsistent. A facility might require four shifts per month, but when a PRN nurse goes three months without picking one up, nothing happens. They stay on the roster, clogging up the pool.
A better model:
- Clear minimums: 4 shifts per month, including at least one weekend
- Transparent consequences: Miss two consecutive months → removed from active scheduling
- Reinstatement path: Re-credential and re-onboard, but don’t hold the spot indefinitely
This isn’t punitive. It’s practical. It creates predictability without adding cost — and it ensures your PRN pool is an actual resource, not a list of names.
The agencies with the healthiest PRN pools enforce their own minimums. The ones drowning in callouts have rosters full of names and nobody picking up the phone.
Coverage First, Time Off Second
In restaurants, time off wasn’t approved until coverage was secured. You had to demonstrate the shift would be filled before the schedule changed.
At Hillstone, I still remember planning around who I could swap with. If I wanted a Saturday off, I’d start working the phones on Monday. Inconvenient but when my day off came, I didn’t feel guilty, and nobody resented me.
Healthcare can’t go quite that far – union contracts, FMLA protections, legitimate emergencies. But the principle holds: make time off a shared planning responsibility.
A realistic healthcare adaptation:
- Staff attempt coverage for non-emergency time-off requests
- If coverage isn’t found within 48 hours, a defined escalation pathway activates: float pool → internal PRN → agency partner
- Last-minute requests without coverage effort move to lower priority for future requests
This shifts the culture from “I put in for the day off, it’s your problem now” to “I’m part of a team, and the schedule is our shared commitment.”
Schedule Consistency Drives Payroll Accuracy
Here’s an angle most people don’t think about: fixed schedules don’t just help with coverage – they help with payroll.
I spent the last seven years of my time at Hillstone as a payroll accountant, and I saw firsthand how schedule consistency translated into payroll accuracy. I worked both sides, as a unit accountant for a specific restaurant, and at the company level processing payroll across locations.
At the restaurant level, if I noticed someone didn’t have hours logged for a shift they were scheduled to work, I’d flag it with the manager before finalizing. At the company level, I could spot patterns, a location consistently underreporting, a department with unusual variances, and ask the right questions before payroll went out the door.
We ran extensive testing before every payroll cycle to catch missed hours, duplicate entries, and scheduling discrepancies. The result? Fewer corrections, fewer underpayments, and fewer compliance headaches.
In healthcare, this principle scales:
- Fixed scheduling frameworks make it easier to reconcile hours against time systems
- Predictable patterns help payroll teams spot anomalies before they become corrections
- Fewer last-minute schedule changes mean fewer manual payroll adjustments — and fewer errors that erode employee trust
When nurses don’t trust that their hours will be captured accurately, it damages morale faster than almost any other operational failure. Schedule structure isn’t just a coverage tool — it’s a payroll integrity tool.
What Doesn’t Translate to Healthcare Shift Coverage (And Why That’s Important)
The restaurant model doesn’t translate wholesale. The benefits structure at a restaurant is leaner than what healthcare demands for 12-hour clinical shifts. Firing for a single callout is a legal minefield. Ignoring overtime isn’t an option when it’s one of the largest controllable labor costs on a healthcare P&L.
But here’s the trap: healthcare often overcorrects so far in the other direction that there are no meaningful consequences at all.
A nurse calls out six Fridays in a row and nothing happens. Core staff absorb it. Morale tanks. Retention drops. That single pattern of avoidable absenteeism compounds into turnover costs that most leaders dramatically underestimate.
The Real Lesson: Structure Creates Flexibility
Here’s the paradox healthcare often misses:
The more structured your scheduling rules are, the more flexible your workforce becomes.
Hillstone didn’t have flexibility because they were lenient. They had it because expectations were crystal clear. Everyone knew the minimum, the coverage rule, and the consequences. And within that framework, people figured it out — swapped shifts, traded weekends, covered for each other, and made it work.
Healthcare leaders often try to “be flexible” by bending rules. What they actually end up with is:
- Repeat schedule gaps nobody owns
- Overworked core staff carrying the weight
- Burned-out managers rebuilding the schedule every week
- Expensive last-minute agency fixes
Clear expectations, shared responsibility, and consistent follow-through. That’s the formula, whether you’re running a Friday night dinner rush or a 36-bed med-surg unit.
A Question Worth Asking in 2026
Instead of asking:
“Why won’t staff commit to the schedule anymore?”
Try asking:
“Have we built a system that makes commitment possible – and rewarding?”
People don’t avoid responsibility. They avoid unclear, unfair, and inconsistent systems. They avoid environments where the nurse who calls out every Friday faces no consequences while the nurse who never misses gets no recognition.
At ATC Healthcare, we’ve spent decades helping facilities build staffing models that aren’t just reactive, they’re structural. As the #7 per diem nursing agency nationally, we see what works and what doesn’t across hundreds of units, thousands of shifts, and every type of clinical environment.⁶
The facilities that win aren’t the ones with the biggest PRN pools. They’re the ones with the clearest expectations, the fairest systems, and the partners who help them fill the gaps before they become crises.
Final Thought
Healthcare doesn’t need to become a restaurant.
But it does need to stop pretending that chaos is the cost of caring.
Structure is not the enemy of compassion. It’s what protects it.
Want to know what your callout patterns are really costing you?
ATC Healthcare offers a complimentary coverage analysis for facilities ready to move from reactive staffing to structural solutions. We’ll map your callout frequency, overtime spend, and agency dependency — and show you exactly where schedule structure could save you money while improving nurse retention.
Request your free coverage analysis →
Sources
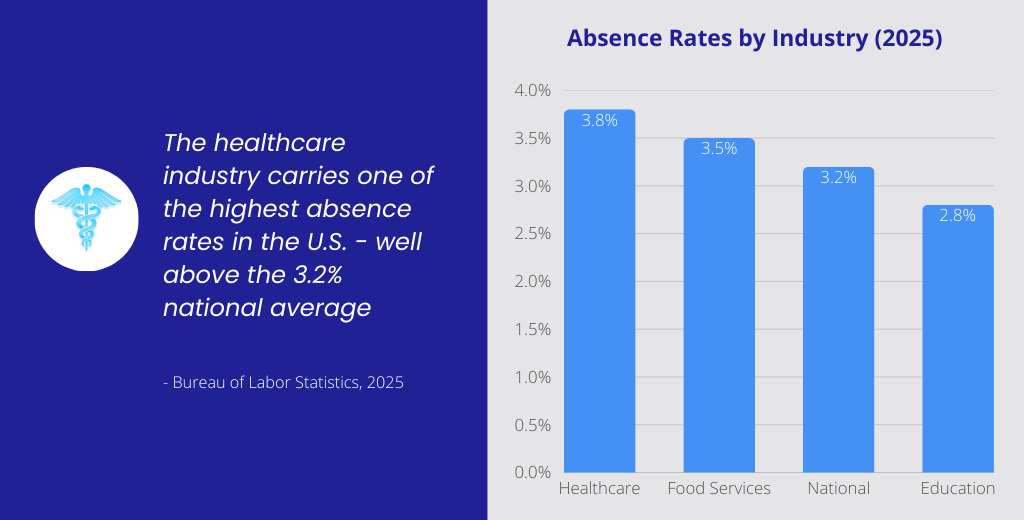
- Bureau of Labor Statistics — Absences from Work, 2025
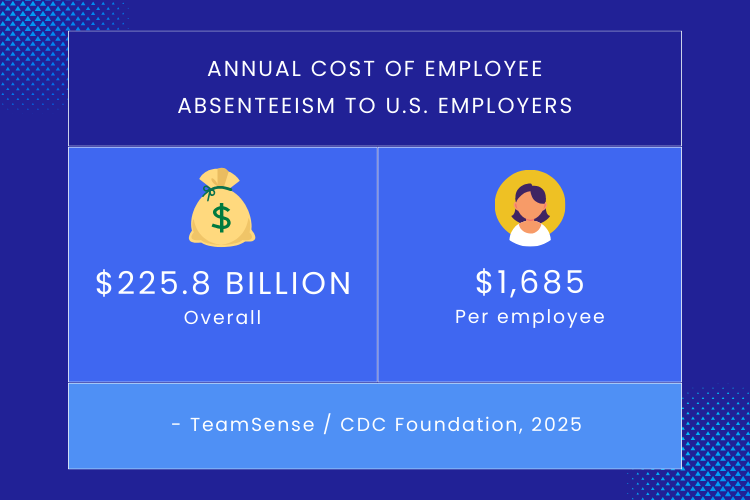
- TeamSense / CDC Foundation — Employee Absenteeism Statistics
- NSI Nursing Solutions / NurseRegistry — Healthcare Staffing Costs, 2024
- ShiftMed — Flexible Scheduling for Nurses, October 2025
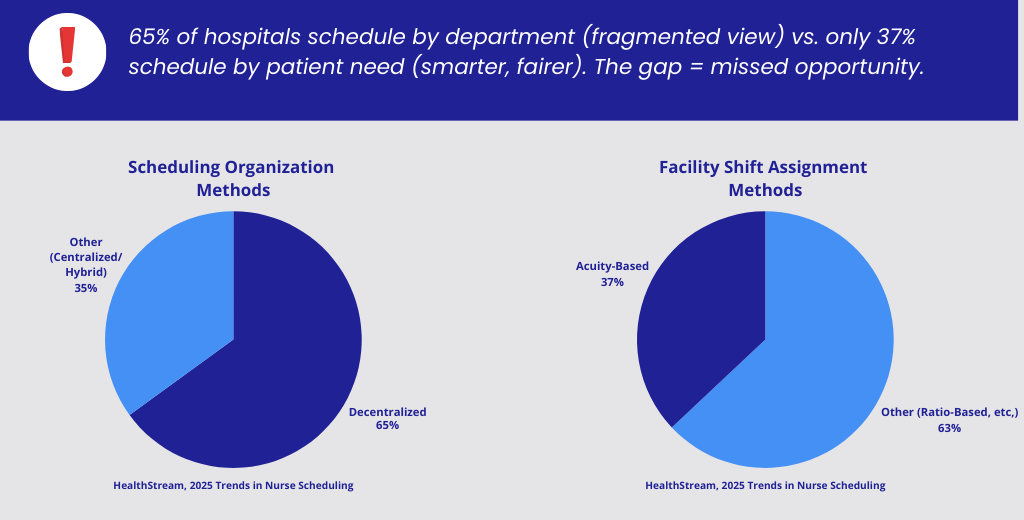
- HealthStream — 2025 Trends in Nurse Scheduling
- SIA — Largest U.S. Staffing Firms, 2025
- NSI / Becker’s Hospital Review — Nurse Turnover Costs, 2025
- HireQuest — Restaurant No-Call/No-Show Costs, 2024
- Interstaff / HealthStream — Scheduling Solutions, 2025