People ask me what PRN nursing actually looks like. After years in healthcare staffing, I’ve learned the best answer is a week in the life of a PRN nurse.
What follows is a composite, built from real conversations with real nurses who choose per diem work through ATC Healthcare. The details are drawn from patterns I’ve seen across thousands of shifts and hundreds of nurses. The experience is real. The week is illustrative.
MONDAY — “The School Play”
It’s 8:15 in the morning and I’m sitting in an auditorium watching my daughter play a talking tree. (Why they would schedule a school play this early in the morning is beyond me!) OMG, she looks so cute. She was so nervous — we were up late last night practicing her lines. I saw some open shifts on the app I could have picked up but I would so much rather be here. These are the moments that make life worth living! I know I’m going to hear about this play (and all the gossip) for 3 days straight. lol Anyway, I think I’ll probably pick up a shift tomorrow – we need the money! #summervacation
TUESDAY — “Twelve Hours”
So I picked up a shift at ABC Hospital today – Med-surg floor, of course. My bread and butter. Walked into five patients. One discharge (yay, paperwork 🙄), one came in overnight with a GI bleed, one post-op knee replacement and TERRIFIED to stand up, and two were stable but complicated — you know, the ones where you actually have to read the whole chart and not just skim it.
The first 90 minutes were busy (like usual). Reading histories I’ve never seen, on a unit I haven’t been on in two weeks, with staff who kinda remember me? Maybe? Assessing, prioritizing, building rapport with patients who are like “great, another new nurse.” It was A LOT.
But by mid-morning I got my rhythm. Got the knee replacement guy up and walking the hall – that’s my win for today. 💪 Provider rounds, new orders, the usual juggle.
By 7:15 PM I’m sitting in my car in the parking garage for like 90 seconds of pure silence before I drive home. (If you know, you know.)
I’m really digging this PRN deal. I read somewhere that nurses who pick their own schedules have way less burnout.² I believe it. The version of me that got mandated into overtime at my old job? She was a completely different woman.
WEDNESDAY — “Off. Actually Off.”
No work today. Yay! And I mean ACTUALLY not working. Not “on call.” Not “available.” Not “well maybe if they really need me.” OFF off.
Finally went to the dentist – I rescheduled that appointment like three times when I was full-time. Took the dog to the park. Did meal prep for the week (or tried to… YouTube lied to me again 😂). Watched two episodes of something that requires absolutely zero medical knowledge.
I love days like this. Where nobody can guilt you, mandate you, or hit you with the “hey, I know you’re off but could you maybe come in for just a few hours?” NO. I’m OFF. 🙅♀️
Honestly, the ability to say no is so important. No rigid system. Just flexibility that IS the system.³
THURSDAY — “Different Hospital, Same Energy”
Went to a different hospital today and got to work on a Tele floor – it keeps me on my toes (and my resume stacked!) I picked up this facility a few weeks ago and liked it enough to keep coming back. It’s about an hour drive (with traffic of course) but that’s ok – I get to listen to those fantasy books I would never admit to anyone!
Anyway, this place has a different EHR (ugh), different unit culture, different coffee situation (worse… but they have those fancy cold brews in the vending machine so it evens out). The staff is really nice though – I setup a play date for my daughter with another nurse who has a daughter the same age. It should be fun – we’re going to go to the park around the corner. Turns out she lives near us.
By 7 PM I was handing off to night shift and driving home with the windows down. Not a bad Thursday. 🌅
What I’ve noticed by working multiple hospitals is that you learn to read a room FAST. I’ve seen how different facilities handle a rapid response. I know which EHR layouts hide the important stuff and which ones surface it. I pick up things I’d never learn working one unit for ten years. PRN makes me a much more adaptable nurse. I kind of feel like Wonder Woman!
FRIDAY — “The 5:31 AM Text”
Got woken up at 5:31 AM this morning. (I really need to learn to put my phone on vibrate!) But it worked out. There was a facility about 30 minutes away that had a callout on day shift. Med-surg. PREMIUM RATE. 💰💰
Mental math took about 30 seconds: drive time — fine. School drop-off — my mom can handle it. Energy level — slept great after yesterday’s shift. I tapped “Accept” before I was even fully awake lol.
💰 Agency per diem RN rates are **$40–48/hr** nationally — experienced nurses in high-demand markets regularly earn **$55+/hr** before premium or surge pay. *— Salary.com / Glassdoor, 2025–2026*
These premium shifts can add serious cash that literally wasn’t in the budget 24 hours ago. You can’t plan for these but when they pop up… you take them. 😏
I get there at 6:55, get report by 7:10, with patients by 7:30. Standard day, nothing crazy. By 7:30 PM I’m driving home knowing that today alone paid what would have taken me two full days at my old staff rate.
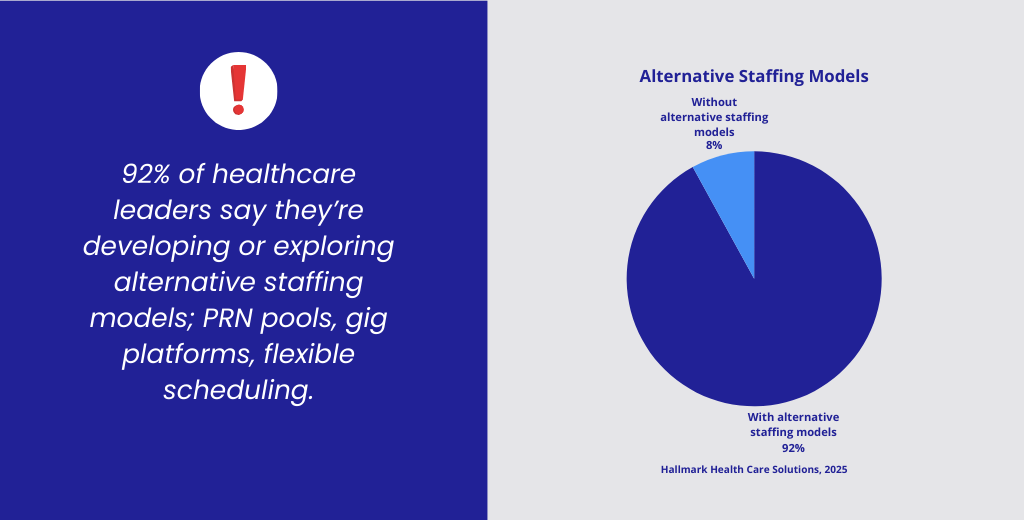
That’s not a trend. That’s the future. And honestly, we’re already living in it.
WEEKEND — “The Pool Wins”
Saturday morning. Kitchen table. Pancakes. No alarm. It was bliss.
I knew there was an evening shift paying time and a half but decided to just be a mom for the day. Spent the day with the kids at the pool. Got a little sunburnt – oops. But got some good family time in and I know the kids really appreciate me making them my priority.
I finally got cleared on another staffing app – praise god. Why is that process so complicated! Ugh. Anyway, I saw a stat the other day – 28% of nurses now work exclusively through staffing platforms, picking their own shifts, facilities, and schedules.⁸ And 67% of clinicians say they’d CHOOSE a temporary role over a permanent one.⁹
What I’ve discovered is that these aren’t nurses who couldn’t find real jobs. (I hate when people say that.) These are nurses who decided that controlling their own time is worth more than a benefits package they can put together themselves anyway.
This is work-life balance – not the corporate retreat version where someone gives a TED talk about it. The REAL version. The Monday morning version where you watch your kid be a talking tree because you built a career that lets you. ❤️
Well – that’s it for the week. I’ve got another shift tomorrow – you know weekends are never 100% free. When someone tells me have a good weekend, I usually want to tell them I’m working but what good would that do?
THE WEEK — SEEN WHOLE
📋 36 hours / 3 shifts / 3 facilities. No mandatory overtime, guilt about the days off, or a single manager deciding my fate.
| Day | What Happened |
| Monday | Watched my daughter’s play. Turned down shifts. Zero regrets. |
| Tuesday | 12 hrs, ABC Hospital, med-surg. Chose it. Crushed it. |
| Wednesday | Actually off. Dentist, dog park, couch. |
| Thursday | 12 hrs, Hospital B, tele. Different hospital, still growing. |
| Friday | 12 hrs, premium callout. 💰 One day = two days of staff pay. |
| Weekend | Pool with the kids. Movie night with loads of junk food. The end. |
A paycheck that matches my value. A schedule that matches my life. And I showed up to every single shift because I WANTED to be there.
That’s one week. Every nurse’s week looks different – and that’s the whole point.
ATC Healthcare has been building this model for decades. We’re not just filling shifts, but rather, building relationships between nurses and the facilities that need them. When a PRN nurse accepts a shift through ATC, she walks into a facility that knows her, a unit that’s expecting her, and a role matched to her skills.
Flexibility isn’t a perk you offer to attract nurses. It’s the reason they stay.
For nurses: Your schedule should work for your life — not the other way around. Browse open PRN shifts near you →
For facilities: The strongest PRN rosters aren’t built in a crisis. Request a staffing consultation →
Sources
- https://www.amergis.com/resources/prn-app-based-nurse-staffing-transforming-healthcare/
- “Scheduling Is Everything”: A Qualitative Descriptive Study of Job and Schedule Satisfaction of Staff Nurses and Nurse Managers – PubMed
- The impact of electronic and self-rostering systems on healthcare organisations and healthcare workers: A mixed-method systematic review – PubMed
- Home | NURSECOMPACT
- Rn Per Diem Salary, Hourly Rate (March 01, 2026) in the United States | Salary.com
- 2025 Healthcare Workforce Trends: A Deep Dive – Hallmark Health Care Solutions